Ideal for: Tumor heterogeneity, patient avatar co-clinical trials
Human cancer xenografts in rodents can provide predictive data on the success of candidate drugs in clinical trials and have been a pivotal tool in moving new drugs from the bench to the clinic. However, currently available immunodeficient mouse models have shown some limitation and variability in tumor take rates and growth kinetics.
Patient Derived Xenograft (PDX), in which tumor tissue is transplanted directly into rodents after biopsy from the patient, allows for better modeling of the molecular features, heterogeneity, and pathology of the original tumor and for predicting treatment sensitivity. Additionally, it allows for the generation of models for tumor types that have not been amenable to cell line generation. Despite the many advantages of this approach for preclinical research, PDX mouse models are hindered by low engraftment rates and slow tumor growth kinetics. The loss of patient tumor heterogeneity and stromal cells as the PDX is passaged multiple times to generate sufficient tumor tissue to perform efficacy studies is also a disadvantage.
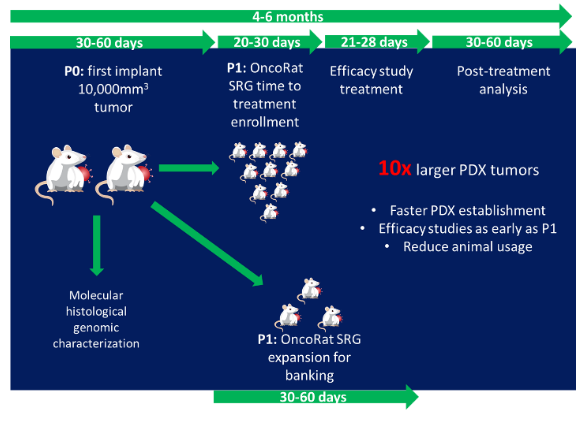
To address these limitations, we have demonstrated that the OncoRat has impressive tumor take rates and growth kinetics for non-small cell lung cancer (NSCLC) PDXs. The NSCLC PDXs in the OncoRat allow for large tumor volume growth, over 20,000 mm3 in the first passage (P0) in the rat, which provides an ample source of tissue for characterization and/or subsequent passage (P1) into OncoRat or mouse for drug efficacy studies. Fewer animals are used for the study with faster timelines to drug efficacy data. In addition, we have used genomic analysis to direct a precision medicine approach. One of our NSCLC PDX models harbors a novel activating MET mutation pathway, which would predict responsiveness to type II MET inhibitors. An efficacy study we performed in NSG mice engrafted with OncoRat produced PDX models confirmed this hypothesis as this PDX was highly responsive to the Type II MET inhibitors, but not to Type I. This proof of concept study demonstrates that genomic and molecular analysis can provide actionable insight to guide treatment decisions and that PDX models established in the OncoRat could serve as a unique platform to aid in therapeutic translation.
Timeline and schematic for PDX establishment, characterization, and efficacy study
OncoRat PDX products & services
- Xenograft efficacy studies, including collection of blood, tissues and tumor for ADME, PK/PD and analysis.
- PDX models and OncoRats off-the-shelf for engraftment at the customers facility.
- New PDX model establishment
- Patient avatar co-clinical trial studies
- Weekly or bi-weekly tumor sampling via fine need aspiration (FNA). For longitudinal evaluation of drug exposure, histology and gene expression.
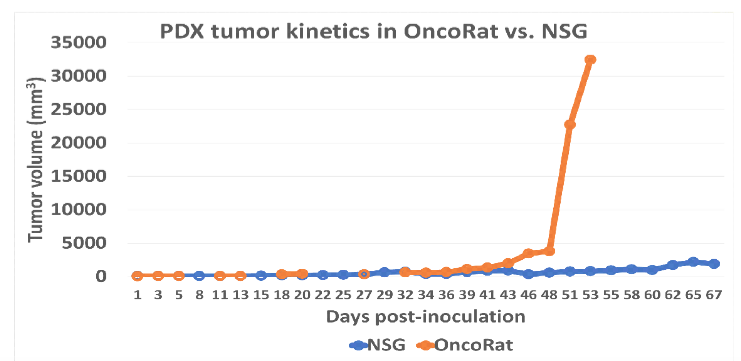
PDX Tumor Kinetics
NSCLC PDX patient 3010 histology and genetic mutation identification
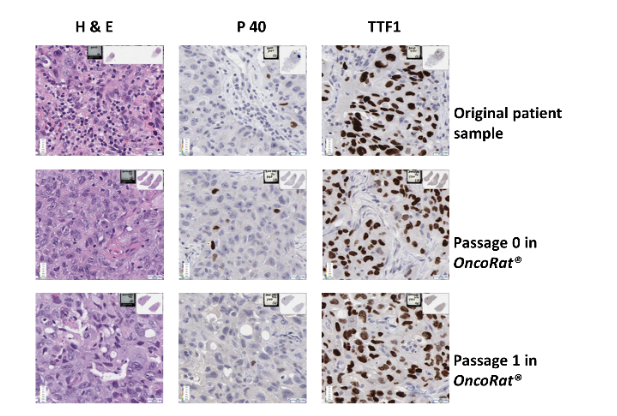
IHC staining for H&E, P40, and TTF1 in original patient tumor sample, first passage (P0) and second passage (P1) in the OncoRat.
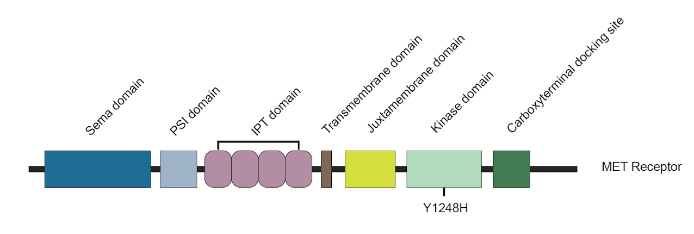
Schematic of MET receptor depicting the likely pathogenic mutation Y1248H found in patient 3010.
Drug efficacy in NSCLC PDX model with patient 3010
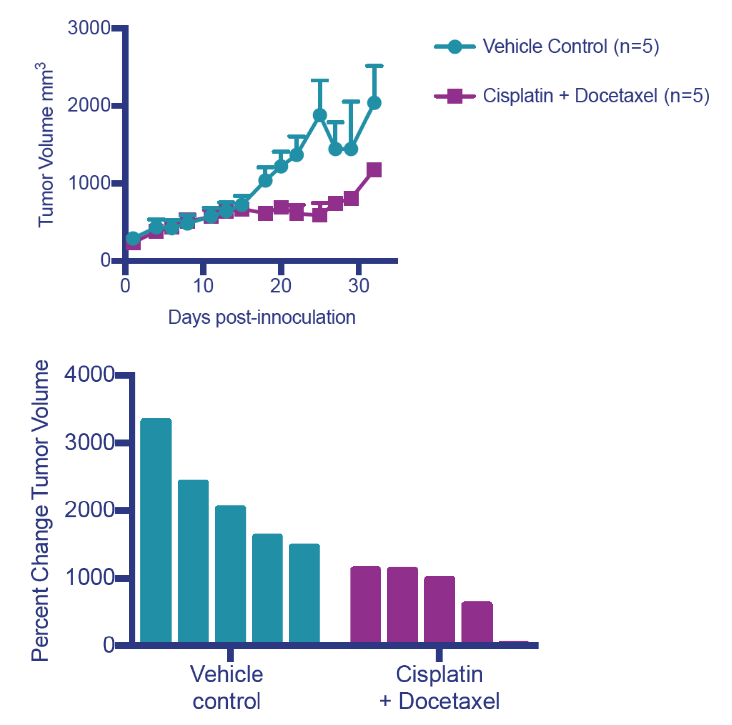
Tumor growth curve and waterfall plot of patient derived NSCLC tumors (3010)
Additional efficacy data in NSCLC PDX model with patient 3010
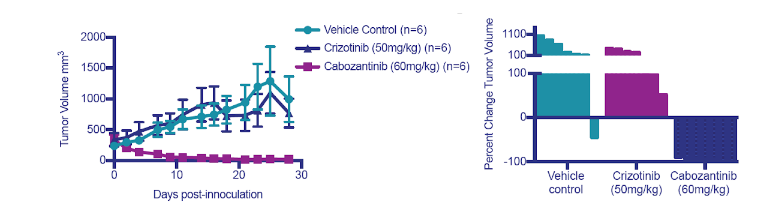
Tumor growth curve and waterfall plot of patient derived NSCLC tumors (3010)
Molecular analysis of PDX efficacy study
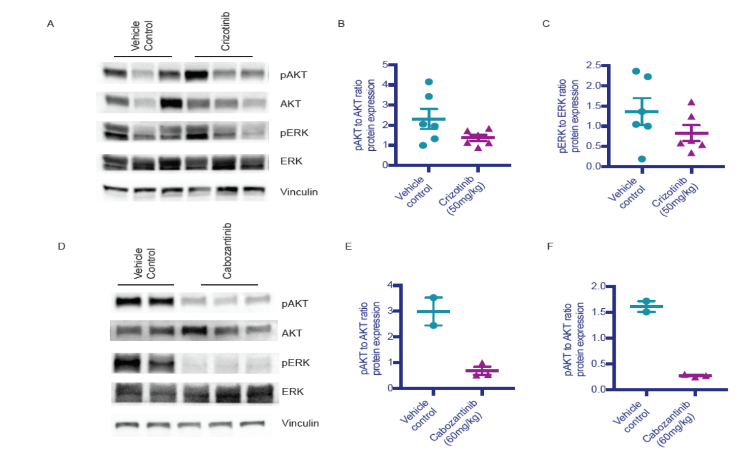
A) Western Blot analysis for phosphorylated AKT, AKT, phosphorylated ERK, ERK, and Vinculin in PDX model treated with vehicle control or drug. Quantification of densitometry depicting ratio of B) phosphorylated AKT to total AKT and C) phosphorylated ERK to total ERK. D) Western blot analysis for phosphorylated AKT, AKT, phosphorylated ERK, ERK, and Vinculin in PDX model treated with one dose of vehicle control or drug. Quantification of densitometry depicting ratio of E) phosphorylated AKT to total AKT and F) phosphorylated ERK to total ERK.
NSCLC PDX Models
| NSCLC PDX 3010 | |
|---|---|
| Demographics | Caucasian male, 54years old, Appalachian, current smoker |
| Tumor specifics | NSCLC Adeno; 11 x ~5 mm, invasive, primary cancer; histology type ICDO3-81403-ADENOCARCINOMA, NOS; stage N1/T3 |
| Tumor location | ICDO3-C34-Bronchus And Lung site, with a specific site of ICDO3-C34.8-Overlapping Lesion of Lung and ICDO3-C34.1-Upper Lobe, Lung with right laterality |
| Surgery & PDX specifics | Surgery completed on 11/3/2017; Implanted into the bilateral hindflank of the SRG F (3); 40 min transplant time; fixed and flash frozen |
| Mutation | Occurred in the MET gene; pathogenic variant c.3742T>C (p. Tyr1248His);homozygous. Likely Pathogenic as somatic variant. Tyr1248Asp and Tyr1248Cys are reported in HGMD in Papillary renal carcinoma patients |
| TTF1 | Positive |
| P40 | Negative |
| NSCLC PDX 3095 | |
|---|---|
| Demographics | African American male, 54 years old, current smoker |
| Tumor specifics | NSCLC; invasive, primary tumor; histology type ICDO3-82303-SOLID CARCINOMA, NOS; stage N0/T2b |
| Tumor location | ICDO3-C34-Bronchus And Lung site with a specific site of ICDO3-C34.1-Upper Lobe, Lung with left laterality |
| Surgery & PDX specifics | Surgery completed on 12/7/2017; implanted into the single |
| Mutation | CDKN2A (NM_000077.4) gene; pathogenic variant c. 28G>T (p.Glu10*). Pathogenic Somatic mutation in Squamous cell carcinoma (COSMIC) |